01
Supine Stable Pelvic Bridge
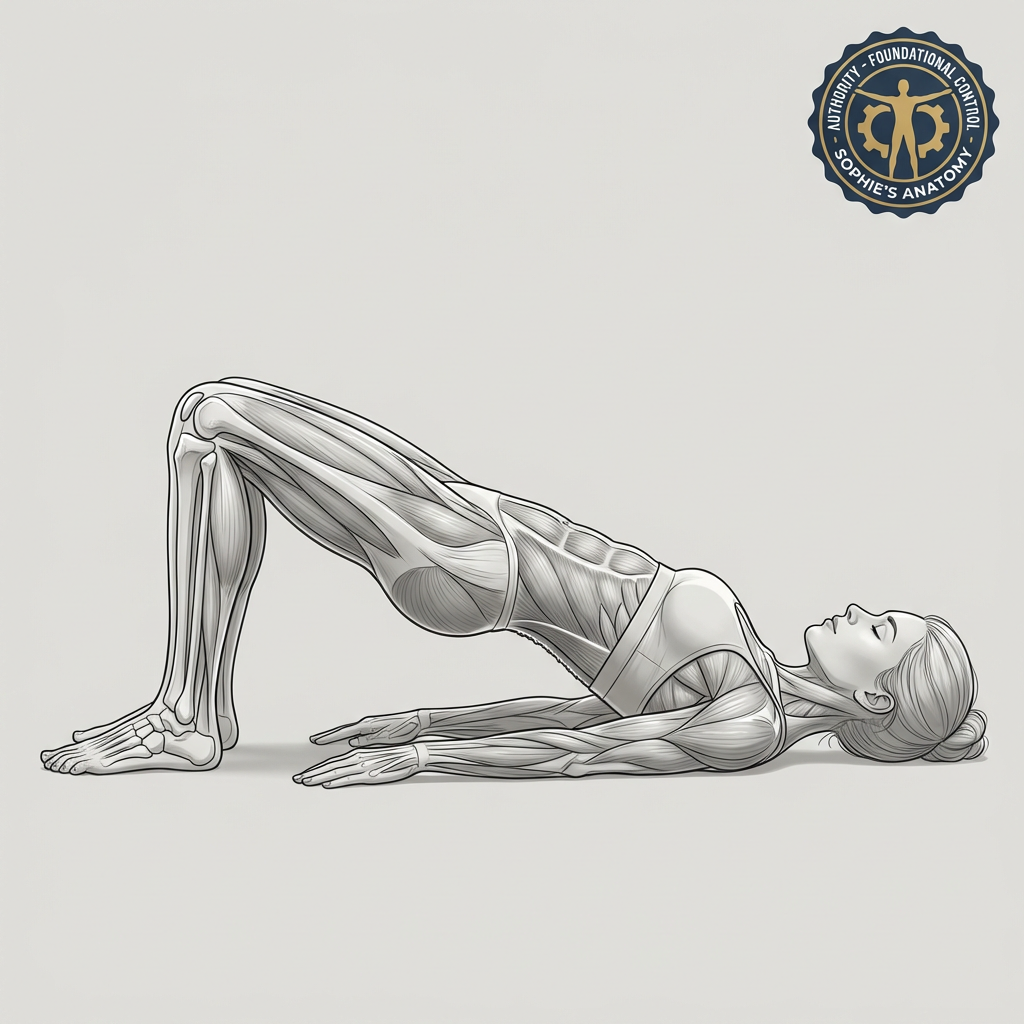
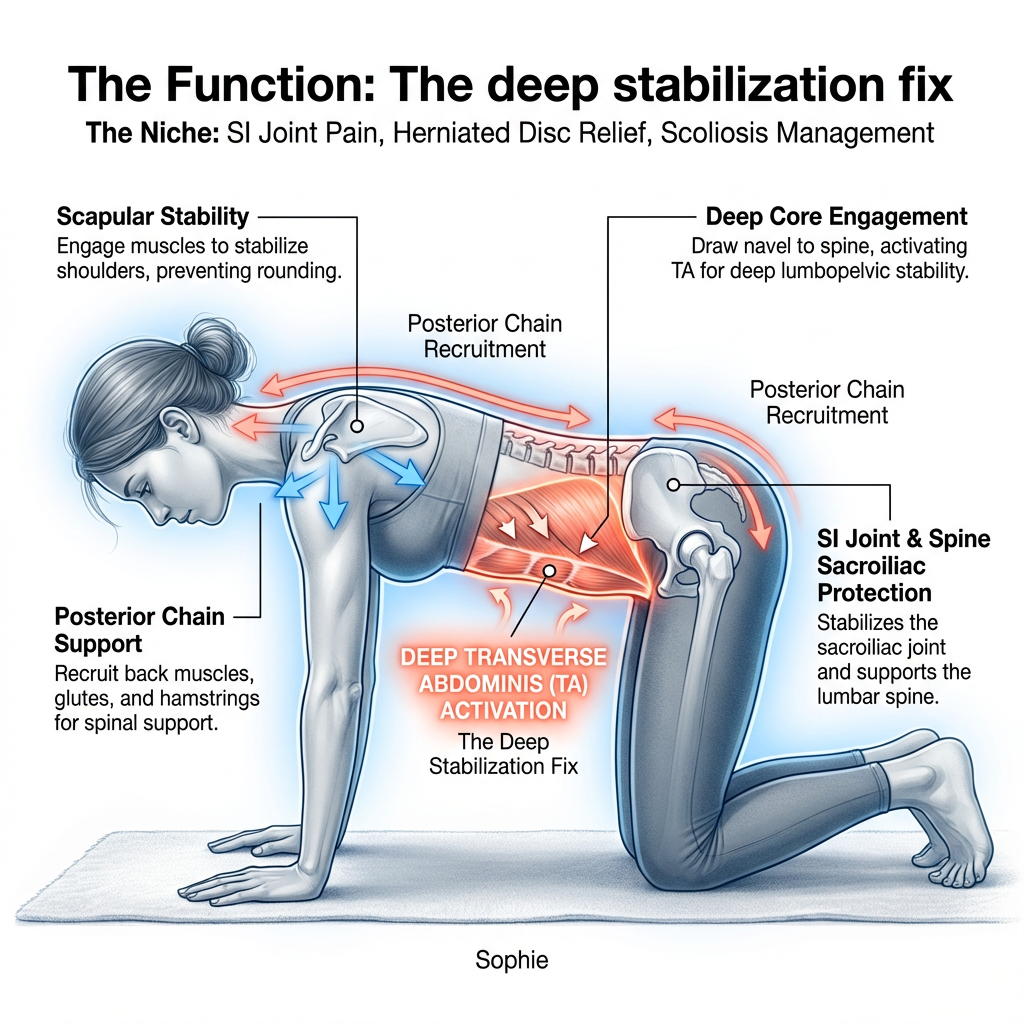
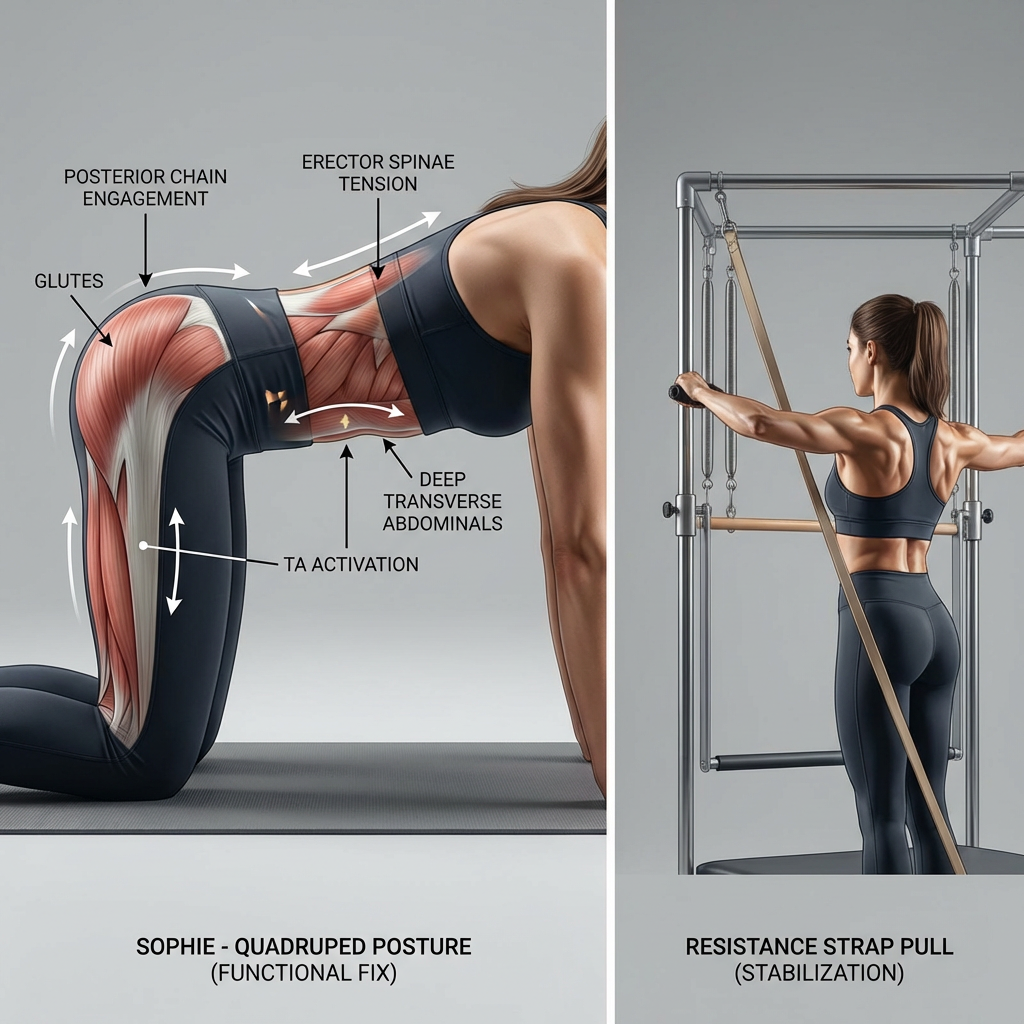
Sophie's Deep Stabilisation Reset — Supine Stable Pelvic Bridge
Standard Stretching
Generic passive stretching bypasses deep stabilisation entirely — temporary relief, no lasting change.
Sophie's Deep Stabilisation Reset Supine Stable Pelvic Bridge — precise, controlled activation that builds the functional stability your body needs.